MDS Study Design
ASCERTAIN: A Phase 3 MDS and CMML clinical trial1
Designed to evaluate the only oral HMA therapy for patients with MDS and CMML1-3
INQOVI is the only oral hypomethylating agent (HMA) therapy approved for adults with intermediate- to high-risk myelodysplastic syndromes (MDS), including chronic myelomonocytic leukemia (CMML).2,3
ASCERTAIN was an open-label, randomized, Phase 3 crossover trial (N=133) that evaluated systemic decitabine exposure, demethylation activity, and safety between INQOVI and intravenous (IV) decitabine in a broad range of adult patients with MDS or CMML.1,2
The trial allowed for intrapatient comparison in the first 2 randomized treatment cycles, then assessment of long-term efficacy and safety of INQOVI as a single arm. Median follow-up was approximately 2.6 years.1,2
Eligibility criteria2
- Diagnosis of MDS or CMML (International Prognostic Scoring System [IPSS] intermediate-1, intermediate-2, or high-risk)
- Treatment naïve or ≤1 prior cycle of decitabine or azacitidine
- No restrictions on body weight or surface area
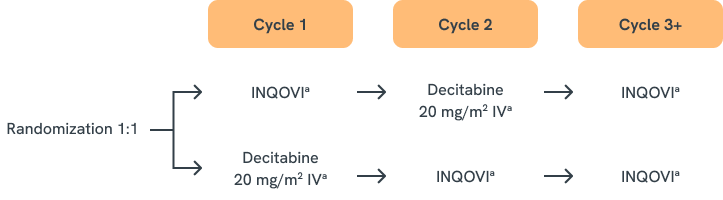
aFive days.
Endpoints evaluated in the ASCERTAIN Phase 3 trial
| ENDPOINTS | PHASE 3 (N=133)1,2 | PHASE 3 LONG-TERM FOLLOW-UP (N=133)1 |
|---|---|---|
| PRIMARY ENDPOINTS | 5-day area under the curve (AUC) between INQOVI and IV decitabine for Cycles 1 and 2 | 5-day AUC between INQOVI and IV decitabine for Cycles 1 and 2 |
| KEY SECONDARY ENDPOINTS |
|
|
| OTHER ENDPOINTS |
|
|
| ENDPOINT | PHASE 3 (N=133)13,14 |
|---|---|
| PRIMARY ENDPOINTS | 5-day under the curve (AUC) between oral decitabine-cedazuridine and IV decitabine for Cycles 1 and 2 |
| KEY SECONDARY ENDPOINTS |
|
| OTHER ENDPOINTS |
|
| ENDPOINT | PHASE 3 LONG-TERM FOLLOW-UP (N=133)1 |
| PRIMARY ENDPOINTS | 5-day AUC between oral decitabine-cedazuridine and IV decitabine for Cycles 1 and 2 |
| KEY SECONDARY ENDPOINTS |
|
| OTHER ENDPOINTS |
|
Patient demographics and disease characteristics at baseline1,2
| BASELINE PATIENT CHARACTERISTIC | PHASE 3 (N=133) |
|---|---|
| AGE (YEARS) | |
| Median (range) | 71 (44-88) |
| SEX (%) | |
| Male | 65 |
| Female | 35 |
| RACE (%) | |
| White | 91 |
|
Black or African American |
3 |
| Asian | 2 |
| Other or not reported | 4 |
| ECOG PERFORMANCE SCORE (PS) (%) |
|
| 0 | 41 |
| 1 | 59 |
| 2 | 0 |
| DISEASE CATEGORY/IPSS (%) | |
| MDS intermediate-1 risk | 44 |
| MDS intermediate-2 risk | 20 |
| MDS high-risk | 16 |
| MDS low-risk | 8 |
| CMML | 12 |
| PRIOR HMA THERAPY (%)a | |
| Prior azacitidine | 5 |
| Prior decitabine | 3 |
| TRANSFUSION DEPENDENCE (%)b | |
| RBC transfusion dependence | 39 |
| Platelet transfusion dependence | 8 |
aOne cycle only, per the exclusion criteria.
bDefined as documentation of ≥2 units of transfusion within 56 days of the first day of study treatment.
References: 1. Garcia-Manero G, McCloskey J, Griffiths EA, et al. Oral decitabine-cedazuridine versus intravenous decitabine for myelodysplastic syndromes and chronic myelomonocytic leukaemia (ASCERTAIN): a registrational, randomised, crossover, pharmacokinetics, phase 3 study. Lancet Haematol. 2024;11(1):e15-e26. 2. INQOVI [package insert]. Princeton, NJ: Taiho Oncology, Inc.; 2026. 3. Zeidan AM, Perepezko K, Salimi T, Washington T, Epstein RS. Patients’ perspectives on oral decitabine/cedazuridine for the treatment of myelodysplastic syndromes/neoplasms. Ther Adv Hematol. 2024;15:20406207241257313.