INQOVI is an oral HMA composed of decitabine and cedazuridine1
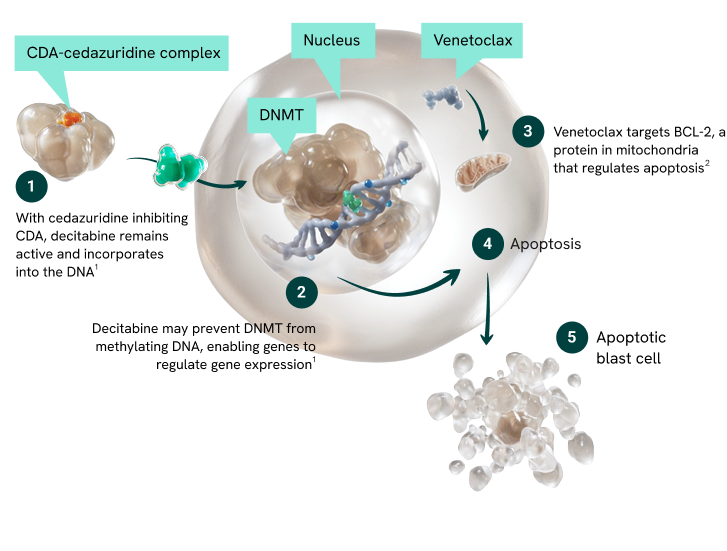
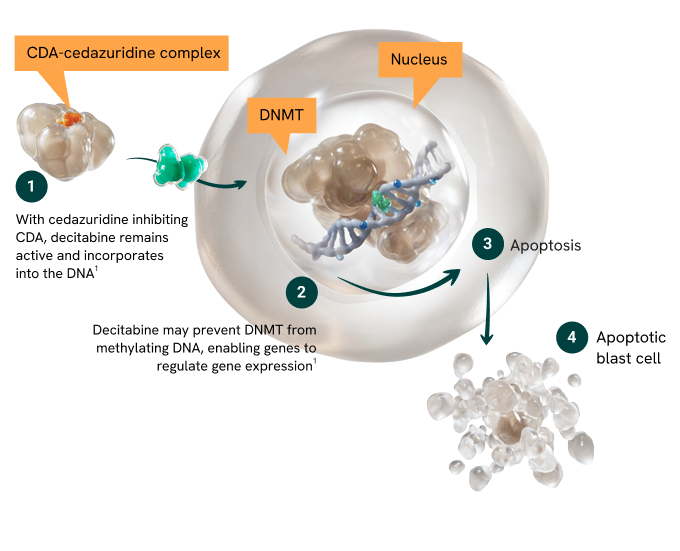
Decitabine is a nucleoside analog that incorporates into DNA and inhibits DNA methyltransferase (DNMT), resulting in DNA hypomethylation and reactivation of silenced genes, including those regulating cellular differentiation and apoptosis1
Cedazuridine inhibits cytidine deaminase (CDA), an enzyme in the liver and gut that rapidly degrades decitabine, thereby increasing systemic exposure and enabling oral delivery1
Proposed MOA for INQOVI + venetoclax in AML
For illustrative purposes only. Not intended to imply clinical significance.
Together, INQOVI and venetoclax promote apoptosis in AML cells by reactivating silenced apoptotic pathways and directly inhibiting survival signals.1-3
Proposed MOA for INQOVI in MDS
For illustrative purposes only. Not intended to imply clinical significance.
AML efficacy
INQOVI + venetoclax delivered consistent exposure and meaningful response.1,4
References: 1. INQOVI [package insert]. Princeton, NJ: Taiho Oncology, Inc.; 2026.
2. VENCLEXTA [package insert]. North Chicago, IL: AbbVie Inc. and South San Francisco, CA: Genentech, Inc.; 2026.
3. Bouligny IM, Murray G, Doyel M, et al. Venetoclax with decitabine or azacitidine in the first-line treatment of acute myeloid leukemia. eJHaem. 2023;4(2):381-392.
4. Data on file. Taiho Oncology Inc., Princeton, NJ.
5. Garcia-Manero G, McCloskey J, Griffiths EA, et al. Oral decitabine-cedazuridine versus intravenous decitabine for myelodysplastic syndromes and chronic myelomonocytic leukaemia (ASCERTAIN): a registrational, randomised, crossover, pharmacokinetics, phase 3 study. Lancet Haematol. 2024;11(1):e15-e26
IMPORTANT SAFETY INFORMATION
IMPORTANT SAFETY INFORMATION
WARNINGS AND PRECAUTIONS
Myelosuppression INQOVI as Monotherapy for MDS or CMML
In patients with MDS or CMML, INQOVI can cause severe myelosuppression, including fatal adverse reactions. Based on laboratory values, new or worsening thrombocytopenia occurred in 82% of patients, with Grade 3 or 4 occurring in 76%. Neutropenia occurred in 73% of patients, with Grade 3 or 4 occurring in 71%. Anemia occurred in 71% of patients, with Grade 3 or 4 occurring in 55%. Febrile neutropenia occurred in 33% of patients, with Grade 3 or 4 occurring in 32%. Thrombocytopenia, neutropenia, anemia, and febrile neutropenia are the most frequent cause of INQOVI dose reduction or interruption, occurring in 36% of patients. Permanent discontinuation due to myelosuppression (febrile neutropenia) occurred in 1% of patients. Myelosuppression and worsening neutropenia may occur more frequently in the first or second treatment cycles and may not necessarily indicate progression of underlying MDS.
Fatal and serious infectious complications can occur with INQOVI. Pneumonia occurred in 21% of patients, with Grade 3 or 4 occurring in 15%. Sepsis occurred in 14% of patients, with Grade 3 or 4 occurring in 11%. Fatal pneumonia occurred in 1% of patients, fatal sepsis in 1%, and fatal septic shock in 1%.
Obtain complete blood cell counts prior to initiation of INQOVI, prior to each cycle, and as clinically indicated to monitor response and toxicity. Administer growth factors and anti‑infective therapies for treatment or prophylaxis as appropriate. Delay the next cycle and resume at the same or reduced dose as recommended.
INQOVI in Combination with Venetoclax for AML
In patients with AML, INQOVI can cause severe myelosuppression, including fatal adverse reactions, when given in combination with venetoclax. Based on laboratory values in Study ASTX727-07, Phase 2 new or worsening thrombocytopenia occurred in 70% of patients, with Grade 3 or 4 occurring in 69%. Neutropenia occurred in 48% of patients, with Grade 3 or 4 occurring in 48%. Anemia occurred in 54% of patients, with Grade 3 or 4 occurring in 50%. Febrile neutropenia occurred in 52% of patients, with Grade 3 or 4 occurring in 52%. Thrombocytopenia, neutropenia, anemia, and febrile neutropenia were a frequent cause of INQOVI and/or venetoclax dose reduction or interruption. Dose reductions of INQOVI due to neutropenia and thrombocytopenia occurred in 4% and 1% of patients, respectively. Dose interruptions of INQOVI due to neutropenia, febrile neutropenia, thrombocytopenia, and anemia occurred in 40%, 11%, 8%, and 2% of patients, respectively.
Fatal and serious infectious complications can occur during treatment with INQOVI and venetoclax. Pneumonia occurred in 25% of patients, with Grade 3 or 4 occurring in 20%. Sepsis occurred in 28% of patients, with Grade 3 or 4 occurring in 18%. Fatal pneumonia occurred in 2% of patients and fatal sepsis in 8%.
Obtain complete blood cell counts prior to initiation of INQOVI with venetoclax, prior to each cycle, and as clinically indicated to monitor response and toxicity. Administer growth factors and anti-infective therapies for treatment or prophylaxis as appropriate. Delay the next cycle and resume at the same or reduced dose as recommended.
Embryo-Fetal Toxicity
Advise patients of the potential risk to a fetus. Advise females of reproductive potential to use effective contraception during treatment with INQOVI and for 6 months after the last dose. Advise males with female partners of reproductive potential to use effective contraception during treatment with INQOVI and for 3 months after the last dose.
ADVERSE REACTIONS
INQOVI as Monotherapy for MDS or CMML
Serious adverse reactions occurred in 68% of patients who received INQOVI. Serious adverse reactions in >5% of patients included febrile neutropenia (30%), pneumonia (14%), and sepsis (13%). Fatal adverse reactions occurred in 6% of patients. These included sepsis (1%), septic shock (1%), pneumonia (1%), respiratory failure (1%), and one case each of cerebral hemorrhage and sudden death.
The most common adverse reactions (≥20%) were fatigue (55%), constipation (44%), hemorrhage (43%), myalgia (42%), mucositis (41%), arthralgia (40%), nausea (40%), dyspnea (38%), diarrhea (37%), rash (33%), dizziness (33%), febrile neutropenia (33%), edema (30%), headache (30%), cough (28%), decreased appetite (24%), upper respiratory tract infection (23%), pneumonia (21%), and transaminase increased (21%). The most common Grade 3 or 4 laboratory abnormalities (≥50%) were leukocytes decreased (81%), platelet count decreased (76%), neutrophil count decreased (71%), and hemoglobin decreased (55%).
INQOVI in Combination with Venetoclax for AML
Serious adverse reactions occurred in 82% of patients who received INQOVI+VEN. Serious adverse reactions in >5% of patients included febrile neutropenia (31%), sepsis (22%), pneumonia (15%), infection (bacterial/viral) (10%), hemorrhage (9%), and dyspnea (6%). Fatal adverse reactions occurred in 8% of patients who received INQOVI+VEN. These included sepsis (5%), dyspnea (2%), myocardial infarction (1%), hemolytic anemia (1%), and tumor lysis syndrome (1%).
The most common adverse reactions (≥20%) were neutropenia (60%), febrile neutropenia (52%), thrombocytopenia (52%), hemorrhage (42%), anemia (41%), infection (bacterial/viral) (40%), diarrhea (38%), fatigue (36%), mucositis (36%), constipation (36%), arthralgia (35%), decreased appetite (31%), edema (31%), nausea (31%), dyspnea (30%), white blood cell count decreased (28%), sepsis (28%), pneumonia (25%), rash (25%), transaminitis (24%), myalgia (23%), arrhythmia (21%), and abdominal pain (21%). The most common Grade 3 or 4 laboratory abnormalities (≥20%) were decreased leukocytes (91%), decreased lymphocytes (81%), decreased platelets (69%), decreased hemoglobin (50%), and decreased neutrophils (48%).
USE IN SPECIFIC POPULATIONS
Lactation
Because of the potential for serious adverse reactions in the breastfed child, advise women not to breastfeed during treatment with INQOVI and for 2 weeks after the last dose.
Renal Impairment
No dosage modification of INQOVI is recommended for patients with mild or moderate renal impairment (creatinine clearance [CLcr] of 30 to 89 mL/min based on Cockcroft-Gault). Due to the potential for increased adverse reactions, monitor patients with moderate renal impairment (CLcr 30 to 59 mL/min) frequently for adverse reactions. INQOVI has not been studied in patients with severe renal impairment (CLcr 15 to 29 mL/min) or end-stage renal disease (ESRD: CLcr <15 mL/min).
Please see full
.
Welcome to the INQOVI® (decitabine and cedazuridine) tablets website
This website is intended for US healthcare professionals only. Are you a healthcare professional in the US?