Dosing Guidance & Modifications
AML and MDS treatment guidelines for INQOVI1
Guidance on taking, monitoring, and adjusting dosing
Indicated dosage: 1 tablet once daily
Fixed-dose combination containing 35 mg of decitabine and 100 mg of cedazuridine
Tablet shown is not actual size. Actual tablet size is 7.94 mm x 14.29 mm.2
Instruct patients to:
Take INQOVI at approximately the same time each day
Swallow INQOVI whole. Do not cut, crush, or chew the tablets
Take INQOVI on an empty stomach at least 2 hours before or 2 hours after eating
If vomiting occurs after dosing, do not take an additional dose, and continue with the next scheduled dose
Skip the dose if more than 12 hours late, take the next scheduled dose, and extend the dosing period by 1 day to ensure 5 daily doses each cycle
Instruct patients also taking venetoclax for AML to:
Take INQOVI and venetoclax at least 2 hours apart. Do not take INQOVI and venetoclax at the same time
Remind patients and their caregivers that INQOVI is a hazardous drug. Follow applicable special handling and disposal procedures. Store at 20°C to 25°C (68°F to 77°F); excursions permitted from 15°C to 30°C (59°F to 86°F).
Monitoring and dose modifications
Guidance on monitoring and dose modifications varies by indication and should be followed accordingly.
Monitoring
- Obtain complete blood cell counts before initiating INQOVI, before each cycle, and as clinically indicated to monitor for response and toxicity
- If patients develop cytopenias, frequently monitor blood cell counts through resolution
- If a bone marrow test is needed, order it as early as Day 22
Dose delays or reductions
Hematologic ARs
If hematologic ARs occur, monitor complete blood cell counts until neutrophils and platelet counts have recovered to Grade 1 or 2 (an absolute neutrophil count [ANC] of ≥1000/μL and platelets of ≥50,000/μL).
If hematologic recovery does not occur within 2 weeks of achieving remission:
Delay INQOVI for up to 2 additional weeks
Consider reducing the number of days of INQOVI per cycle according to the table below
Nonhematologic ARs
If nonhematologic ARs occur, reduce the INQOVI dose according to the table below.
Recommended INQOVI dose reductions for ARs
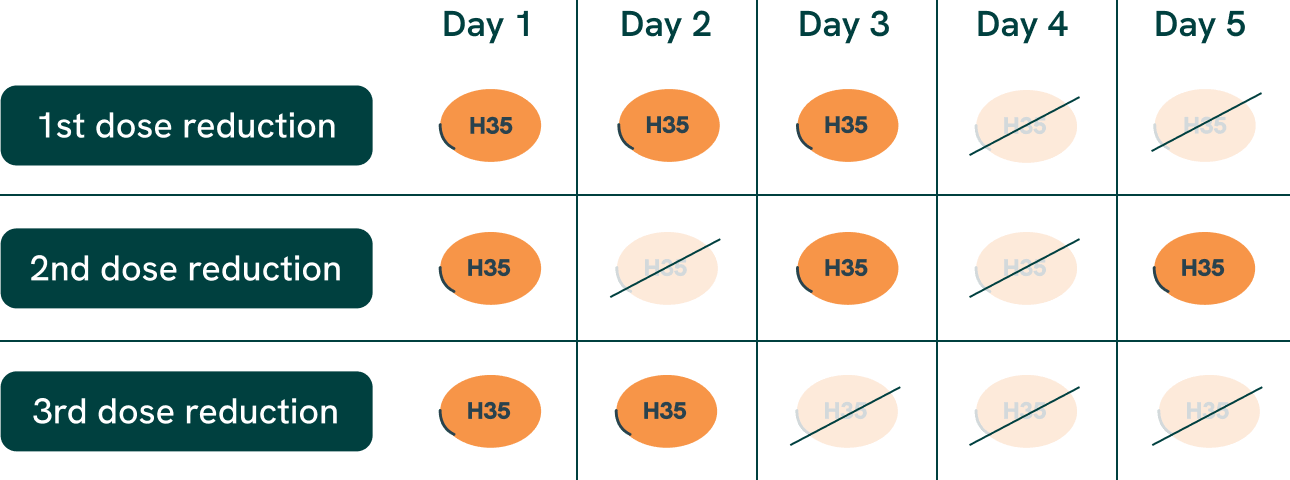
Manage persistent severe neutropenia and febrile neutropenia with supportive treatment.
Monitoring
Obtain complete blood cell counts before initiating INQOVI, before each cycle, and as clinically indicated to monitor for response and toxicity
Dose delays or reductions
Hematologic ARs
Delay the next cycle if absolute neutrophil count (ANC) is <1000 /μL and platelets are <50,000/μL in the absence of active disease. Monitor complete blood cell counts until ANC is ≥1000/μL and platelets are ≥50,000/μL.
If hematologic recovery does not occur within 2 weeks of achieving remission:
Delay INQOVI for up to 2 additional weeks, and resume at a reduced dose by administering INQOVI on Days 1 through 4
Consider further dose reductions if myelosuppression persists after a dose reduction according to the table below
Maintain or increase the dose in subsequent cycles as clinically indicated
Nonhematologic ARs
If the following nonhematologic ARs occur, delay the next cycle, and resume INQOVI at the same dose or at a reduced dose upon resolution:
- Serum creatinine ≥2 mg/dL
- Serum bilirubin ≥2x upper limit of normal (ULN)
- Aspartate aminotransferase or alanine aminotransferase ≥2x ULN
- Active or uncontrolled infection
Recommended INQOVI dose reductions for myelosuppression
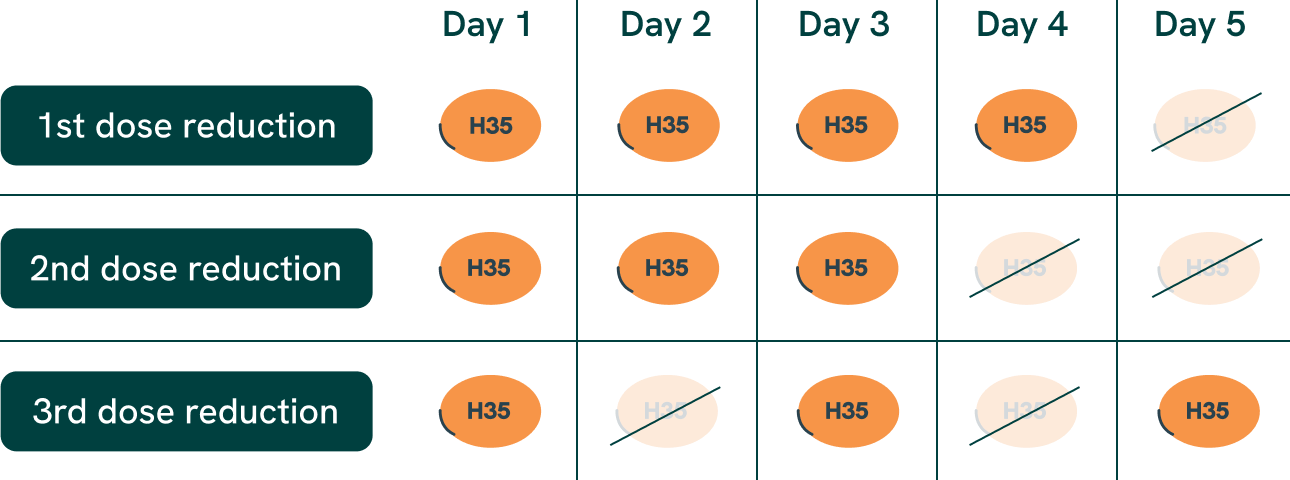
Manage persistent severe neutropenia and febrile neutropenia with supportive treatment.
References: 1. INQOVI [package insert]. Princeton, NJ: Taiho Oncology, Inc.; 2026. 2. Data on file. Taiho Oncology Inc., Princeton, NJ.